Recently a parent put the photograph below on Facebook and asked “Does anyone with or child with aniridia sit this close to the TV to watch it?”
Gabriela watching TV
There was a great set of responses, from all over the world, which are summarised below.
Everyone reported that they/their child sits very close to the screen. Sometimes it is closer than in the photo, sometimes further away, depending up on their visual acuity.
It might be thought that a larger screen would be suitable. This didn’t appear to be the case. In fact often the opposite was true. People with aniridia are usually severely short sighted, so seeing detail at distance is the problem. Enlarging the detail and increasing the distance does not really help and is problematic too.
Katie said “I find that making something twice as big doesn’t necessarily mean I can sit twice as far from it. So even with a large TV I am tempted to sit close. This means if the TV is too large I can’t see all of it at the same time.”
Several people felt that actually small screen on iPads and phones were preferable, to the extent that they don’t use a TV at all.
“Now I have an iPad and can hold it right up to my eye, I rarely ever switch on the TV these days!!”
“Ana didn’t bother with TV till almost 3 years of age, and she prefers to watch Disney on my phone”
“Liam doesn’t even like to watch TV – he prefers his iPad and he holds it a few inches from his face. He sometimes watches the same thing on his iPad that we’re watching on TV! It’s perfect for him. And I love that the other kids aren’t yelling at him to get out of the way when he stands in front of the TV!”
Blocking the view of other people is a common problem. Jenny said “My sisters were constantly shouting ‘Get your head out the way!’ at me when we watched TV together. They would watch from the comfort of the sofa and I sat on the floor!”
Jean commented: “We have had 2 TVs in our lounge since Max – now 13 – was about 3. He has his own TV with a comfortable chair in front of it. It helps him to be able to sit as close as he wants and the other kids and parents don’t have to try and see around him. A practical thing that made it much easier for all of us.”
Jessica said “I used to sit pretty close when I was a kid until I got a hand held monocular when I was 13. When I use it I can sit on the couch like a normal person and watch TV.” However other people reported that this practice was too tiring.
While the floor seems a common place to watch from, a few have found special solutions:
“We got Carson a bean bag, one that’s kind of upright with a back”
“My son sits on the entertainment centre itself so he is right next to the TV!”
“John sits front and centre on a chair I had made for him to reach the exact height of the TV set. I didn’t like him sitting lower holding his neck back.”
The favoured positioning also varied, from central to left or right. “Femke is left eye dominant. She has her own place on the left side of the screen” said Koosje. Jenny explained “I sit side on, rather than facing it, and tilt my head to the left (TV to the right of me) as that’s the best position for my nystagmus (null point). I only have sight in my right eye though. I know children who practically sit upside down to watch the TV as that suits their null point best.
High definition (HD) TVs were not reported to be better than non-HD models. Katie said “I can’t really see the difference between them and ordinary TVs. I think that is because my eyes aren’t capable of seeing the extra details they show, not unless I got really, really close.”
People with aniridia usually do not have stereoscopic vision – the ability to see in the 3D. The reaction to 3D TVs and flims then was at best indifferent, at worse nauseous:
“I have no problem with the 3D at the cinema or the passive glasses systems, but the active glasses systems give me a headache.” – Andrew.
“I visited the temporary SKY 3D tent at Waterloo station about a year ago, and briefly watched something on 3DTV. Within a couple of minutes I was starting to get a headache.” – Keith.
“I went on a motion ride recently and wore the 3D glasses to stop the picture looking blurry.” – Beth.
“I don’t think the 3D effect really worked for me because the vision in one of my eyes is so much better than the other. 3D works by projecting two slightly different images in each eye but the vision in my bad eye is too blurred to notice the difference between the two images so what I see is just the image in my good eye anyway. It didn’t give me a headache though.” – Katie
The best advice overall came from parent Shannon: “Whenever we have bought a new TV, we let Katherine tell us which screen is easiest to see and/or the best for her vision.”
What are your experiences of watching TV? Let us know in the comments below or on the Facebook discussion.
Lois, who has aniridia has been “recognised and commended for her cricketing, determination and courage” at a recent awards evening.
She has benefited from Street Chance a charity initiative to get disadvantaged young people playing cricket and so “increase aspiration, promote mutual respect, and enhance relationships with others”. She is now a top player on the Surrey visually impaired cricket team.
Lois said “Overall I think that my ability to play cricket despite my disability is brilliant opportunity. To be able to mix with other people my own age who do not have a disability and to be treated equally is a wonderful feeling. The fact that I have aniridia does not seem to make a difference to the relationship between me and my cricketing friends.”
“Most of my friends do not notice any difference from me but there them is when it comes to dark or very bright conditions. My friends adapt themselves very well to this and offer to help me out when they realise that I am struggling. I feel that having a disability should not stop any one from succeeding and one should carry on doing what they love no matter what – like I do with my cricket.”
Lois’s coach explained how she plays such a visual game:”When she bowls, the wicket-keeper will clap from behind the stumps to help Lois judge the distance between her and the batter, and if Lois is batting, the bowler will shout play as the ball is released.”
Do you play sport and have a visual impairment? Tell us about it to inform and inspire others about what is possible with aniridia.
We urgently need a keen, reliable volunteer to help us to organise our next conference. How about you?
The Aniridia Network UK Conference 2013 will be in London. Sadly Heather, who did the job last year, unexpectedly has to return to the USA next month. Despite this she has valiantly promised, to do remotely, what she can to set up the event. So we really really need someone to handle things in person here and on the day itself.
Don’t worry if you haven’t planned a conference before or aren’t sure you’d know what to do. The only requirement for volunteering is that you are willing to make the effort to perform the tasks and dedicate some of your personal time to working on it. We will provide the full details of how things were organised last year as a reference.
You would work together with Heather and other volunteers on all aspects of the event including:
Selection and booking of venue plus caterers and childcare services
Liaison with presenters and exhibitors
Publicity and communications with attendees
Registration and payment systems
Evaluation methods
Read the full Conference Officer job description. It is a very exciting role with a huge amount of satisfaction at the end. The gratitude expressed by delegates and knowing the difference the event has made to them is really uplifting. It’ll be an big achievement for you to shout about on a CV too.
Last year’s conference was a massive success. We are eager to improve upon it, but we can’t without your help. Step forward now and be a hero to the whole aniridia community in the UK.
Everyone affected by aniridia, including relatives is invited to join us to find out more about each other and discuss aniridia related topics. James and Heather, two adults with aniridia and volunteers for Aniridia Network UK will be your hosts.
Keith wrote about last year’s event and said: “In one evening, I learnt so much. For the first time felt I have peers who understand my condition – in many cases a hell of a lot better than I do. For the first time I felt supported.”
We know many who couldn’t come last time so hope this time there will be even more people and better still.
Once again it’s fringe event of the Sight Village exhibition running nearby on 6 and 7 November. Sight Village is an excellent event about technology, equipment, and support for people who are blind or partially sighted. If you are going on the 7th and would like to meet someone there who is also affected by aniridia, tell us and we’ll try to put you in touch with other visitors.
We are currently picking a venue for this meet-up but expect it to be a bar which we will ensure it is as accessible as possible. It will start around 6pm and be close to both the exhibition and High Street Kensington Underground station. We can arrange guidance from the station and supply our phone numbers to make getting there as easy as we can.
If you want to come, email meetup@aniridia.org.uk as soon as possible so we know how large a space to reserve. We will then send you the details once arranged. Tell us if you would like to be met at the station.
If you can’t come, how about organising a meet-up of your own? There’s a real appetite around the country for get togethers – it just needs some people to set them up. Contact us for details of how we can help you make it happen near you.
We are looking forward to meeting you. James and Heather
The most decorated paralympian ever has aniridia. She and at least two athletes who have aniridia were at the London 2012 Paralympics. There might also have been a runner and a physiotherapist with aniridia too.
Most decorated
Trischa Zorn from the USA has won the most Paralympic medals in the history of the Games, a total of 55 medals including 41 golds. Her career spanned seven Paralympic Games from 1980 to 2004, across a range of events and categories.
Zorn burst onto the scene at Arnhem in 1980 at the age of just 16, winning five gold medals with world record performances. She set seven world records at Barcelona 1992 as she won 10 golds and 2 silvers. She was chosen to take the Athletes’ Oath at the Atlanta 1996 Games.
At the age of 40 Zorn came out of retirement to compete at the 2004 Athens Games, where she won a bronze in the 100m Backstroke S12 class.
At London 2012 she was among five summer athletes inducted in to the Paralympic Hall Of Fame. It aims to recognise retired athletes and coaches who have a track record of excellent athletic performance, history of fair play and participation in community activities.
Zorn has had iris implants in both eyes. The surgery was done as part of the US Food and Drug Administration’s study of the technique. It was performed by the President of the Cornea Research Foundation of America whose board she later joined. Though also now known as Trischa Zorn-Hudson her website is tirchazorn.com.
London 2012 gold medal winner
MaryFisher is 19 and from New Zealand. At London 2012, her debut Games, she won four medals swimming in most severely visually impaired category. She won the gold and a secured a world record in the 200m Individual Medley. In addition she won silver in the 100m Backstroke and Freestyle events and bronze in the 50m Freestyle.
Goalball
AmandaDennis was in the USA Goalball team at London 2012. They reached the quarter finals before losing 5-0 to China . She comes from Peachtree City in Georgia. She also serves as an ambassador of the US Paralympics movement to promote sports to any and all disabled athletes.
Amanda has been awarded the Helen Copeland Scholarship by the United States Association of Blind Athletes (USABA). It is given to members who are: blind, a student, an athlete and US citizen.
USABA said “When she is not practicing goalball, Amanda is a great student and hopes to attend the University of Georgia to achieve a degree in political science with a concentration in pre-law; she also plans to go on to obtain a master’s degree in law. Amanda has been legally blind since birth due to a hereditary eye condition called Aniridia. Amanda is a great recipient for this scholarship and we cannot wait to see what she does in the future. We wish her all the best with goalball and academics!”
Judo
JustinKarn (aka “The Badger”) is 31 and hails from Canada. At the London 2012 Paralympics he took part in the under 60 kg category but was eliminated from the competition. He started competing when 13 years old .In 2011 he won a bronze medal at the Parapan American Games.
1500 metre runner
Gerrard Gosems from Australia was born in 1970. He competed at Atlanta 1996 in goalball and then in athletics at the Sydney 2000 and Beijing 2008 Paralympics. Although he ran a personal best at the 2011 IPC World Championships it seems he wasn’t in the final Australian London 2012 team.
Visually impaired runners often run with a sighted guide. Gerrard’s was once Sebastian Coe, recently Chair of the London 2012 Organising Committee.
He lives by the philosophy ‘success is a journey, not a destination’, but jokes he has hit many signposts while training”. He has climbed Mount Everest and fallen in to a crevasse because his sherpa forgot to warn him of it.
In 2009 Gerrard took part in the TV show ‘Dancing with the Stars’ and reached the semi-finals.
He got a guide dog at the age of 16 and went on to manage the Vision Australia organisation.
Earlier this year I travelled to the USA to take part in medical research related to aniridia. It and the accompanying holiday was a very special experience.
Background
National Institutes of Health
The National Institutes of Health in the United States of America is made up of 27 institutes. Each has its own medical research agenda but all supporting scientific studies that turn discovery into health. It is based on a large campus in Bethesda, Maryland, just outside Washington DC.
WAGR/11p Deletion Syndrome study
One such study is into a genetic condition called WAGR/11p Deletion Syndrome. It can have many symptoms including aniridia. The study’s purpose is to learn more about how the genes involved can affect those who have the conditions and hence to identify potential treatments. To achieve this, the researchers need to examine 75 people with aniridia as well as people with WAGR/11 Deletion Syndrome. In particular one of the genes that can be affected in the latter condition has been linked to obesity. A genetic factor to obesity could have relevance for the wider human population.
Deciding to participate
Invitations to be involved with in the study had gone out to people with aniridia. Beth and Jenny from Aniridia Network UK took up the offer. I wanted to as well. I have always been keen to learn of and help advance medical understanding of aniridia to benefit me and others. I also saw it as a golden opportunity for me and my wife Zoe to holiday in the USA. NIH would pay for my travel within the USA, so I hatched a plan:
Fly to New York and spend time there.
Fly to Washington DC, stay at NIH, take part in the study while also doing as much sightseeing as possible.
Fly to Chicago and stay with my cousin
Fly home to London.
Preparation
First I had to prove that I actually have aniridia, at a genetic level, not just the physical symptoms of no irises.
I started by writing to various health authorities to request copies of my medical records. This wasn’t easy because many of the places where I was a child patient have since or closed merged with others.
The results said that I am “heterozygous for the mutation c.1080C>T in exon 9 of the PAX6 gene. This mutation changes codon 240 from arginine to a premature STOP codon (p.Arg240X).”
In the rare world of aniridia this is apparently one of its common causes. “Heterozygous” means that like everyone with aniridia I have a pair of PAX6 genes, one normal and one mutated – causing aniridia. The second part means that there is a mutation (spelling error) in the gene’s DNA for what should be an instruction to produce a protein necessary for eye development. Therefore the instructions are nonsense and the protein truncated and the eye doesn’t develop properly.
Meanwhile my parents and I were completing several detailed questionnaires about my and our family’s medical history. Even though Mum has a great memory and many notes this was quite a challenge.
Finally I sent all the papers off to NIH. I was delighted to be accepted into the study. For tourism purposes I declined to go in the depths of the US winter, opting instead for more temperate early April. Eventually the time off work was arranged, travel booked and places to stay organised.
I bought travel insurance independently. I was shocked at the extra premium charged purely because I am visually impaired. Unfortunately there was no way to tell the insurers I would be spending a third of the time away surrounded by the best medical equipment and doctors that money can buy! Thanks to some advice from others via the Aniridia Network UK Facebook page I got as good a deal as possible.
The last thing to do before going was to keep a diary of everything I ate for three days. This would later be analysed by a dietician during the study.
New York
The transatlantic flight was a first for Zoe and me. Neither of us had been outside Europe before. We rented an apartment on East 9th Street – the East Village. Over seven days we had a fabulous time visiting:
The day after landing I got severe neck pain. I could barely move my head without hurting. Via my jujitsu sensei I contacted an excellent therapist. After his massage and acupuncture the problem was almost totally resolved.
National Institutes of Health
I flew to Washington DC two days ahead of Zoe. I booked into The Edmond J. Safra Family Lodge. It’s a slightly odd place with serviced rooms, but self-catering in a communal kitchen, on the NIH campus for patients and relatives to stay for free.
The study took six days plus some overnight stays on the ward. I had engineered a weekend in the middle for tourism. In total I was in Washington DC for nine nights.
Everything was expertly organised by Amanda, the study coordinator. I met the lead researcher, lovely Dr Han a number of times too. The tests were fascinating, varied and a pleasure despite the impositions – admittedly sometimes uncomfortable or even painful. I was the 14th participant to have only aniridia.
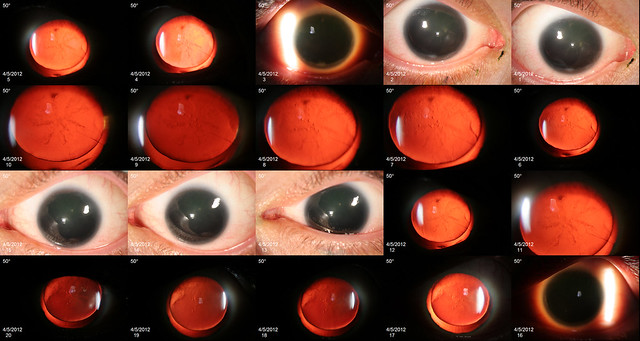
A whole afternoon was dedicated to eye tests to assess: profile vision, acuity, tear production and many other factors. Lots of scanners and cameras were used. The technician had to keep holding my eyes open. They said I had “strong eyelids” but that was clearly code for “non-compliant”! Afterwards though they gave me the amazing imagery they had captured.
I had two stints inside an MRI scanner, once for my skull, the second for my lower abdomen. Again I have the complete set of incredible pictures for posterity. Another scanner provided me with an image of my complete skeleton. All these are unique mementos.
The hearing and auditory processing tests included repeating different words or numbers played into each ear simultaneously. Another involved describing sequences of high or long and low and short notes.
Sense of touch was checked with a thermode – a device held on the skin that can make itself hot or cold. I had to rate the pain induced from none to worst ever! The heat felt more intense to me. I also endured the maximum time permitted, 3 minutes, for holding my hand in very cold water.
To assess smell I was given a booklet full of scratch and sniff panels. For each one I had to identify the odour from a choice of four possibilities. This was quite fun, though as root beer doesn’t exist in the UK, some were a bit tricky!
The psychiatry assessment was stimulating. I had to explain the meanings of words, perform complex mental arithmetic and answer general knowledge questions. The questions relating to US history were a little unfair for an Englishman.
One night I had 25 electrodes glued to my head and more stuck all over my face, chest and legs. I had to sleep like this while a technician monitored me. I didn’t sleep very well but it was easier than I’d feared.
My birthday fell during the study. On that day I was:
woken at 4am and had a plastic bag put over my head for 30mins (to measure CO2 output)
had only a mealshake for breakfast
had 8 blood samples taken
completed a 24 hour urine collection plus gave a further sample
had measurements (height, weight arm span and vital signs) taken twice
got given electric shocks several times in my arms and legs to test my nerves.
On the plus side:
the medical staff got me a cake, card, t-shirt and cap.
I lay in bed till 12:30pm watching Law & Order back to back.
I also got a lunch buffet to test what and how much I chose to eat from a 10,000 calorie spread. I saw this as more of a challenge than a assessment! I regaled Amanda with funny food related anecdotes whilst tucking in.
Finally I got an excellent second massage to fix the stiff but thankfully no longer painful neck I had now had for nearly 2 weeks.
Ordering the hospital food took some mastering. The range of the menu and service was excellent. However the portions were small and they would only deliver precisely what you ordered. Otherwise you’d get cornflakes but no milk for example. I thought I would be safe by requesting a BLT sandwich. But what arrived was a clingfilm wrapped plate with stacked on it: two pieces of toast, lettuce leaves, bacon rashers and tomato slices – in that order. Also I had neglected to order butter for the bread!
Throughout my stay I was shadowed by a man with a video camera. I’d consented to be filmed for a piece on one of the NIH websites. It was interesting watching someone new doing a job my regular colleagues do. Ben was a consummate professional. I’m looking forward to seeing the results on screen.
I was given preliminary results of all the testing before leaving.
Like many with aniridia I have a small pineal gland. It is in the brain and releases a hormone called melatonin that encourages and regulates sleep. Some people with aniridia have reported problems sleeping and so a link to low melatonin levels due to the pineal gland’s size is suspected. My responses to a questionnaire indicate that I don’t have sleep problems though – which is still interesting.
I do though have mild obstructive sleep apnea – I occasionally stop breathing while snoozing which can have serious effects beyond the obvious.
I have relatively good levels of sight compared to other people with aniridia. Dr Han was interested to explore possible genetic reasons for this.
My tears production is fine but the quality of the tears is apparently not. It’s suggested I use eye drops to prevent dry eye.
I have low levels of vitamin D. Dr Han suggested taking supplements – especially since I don’t like being out in the sun, which is normally a source!
I have some hearing loss in my left ear at high frequencies. Obviously I’ll bear it in mind but I’ve never listened to particularly loud music etc. I don’t have Central Auditory Processing Disorder (CAPD).
I’ll look into dealing with these issues in good time.
Everyone on the research team and the ward nurses came to say goodbye at the end. Some of them had been working on my tests behind the scenes so knew me better than I knew them or myself! They had all been so nice and accommodating; I was touched to see them all.
Washington DC
At the weekend and a couple of other times, Zoe and I had time to leave the NIH campus to go into Washington DC together. We mostly walked around seeing:
Capitol Hill
The White House
Washington Monument
Lincoln Memorial
Arlington National Cemetery
Iwo Jima Memorial
Korean War Memorial
Vietnam War Memorial
World War II Memorial
American History Museum
Air and Space Museum
Zoe had more time to explore and also took a day trip to Baltimore to see the aquarium there.
Chicago
We flew out of Washington DC and were met at the airport in Chicago by my cousin Jackie plus her adopted son Matt. It was a short drive to their house in Lake Forest north of the city. They and Jackie’s husband Rob made us very welcome for five days.
We spent some of the time visiting the sights of Chicago. The U-boat in the Science Museum was the highlight for me. But it was too windy for us to go up the tallest tower in America. I liked seeing the elevated train “El” too. The location plus the week in hospital gave me a craving to watch old episodes of ER.
Playing with three year-old Matt was lots of fun too. Zoe and I have a few more catchphrases as a result. It was the first time I’d met my second nephew.
London
All too soon it was time to fly home to London. It had been an amazing trip that gave lots of special memories. Three quite different cities, different places to stay and different reasons to be there. Matt apparently asked when we were coming back, every day for a week after we’d left.
The last thing to do was to use the kit that NIH had provided, to send them four small test tubes of final urine samples. This was to measure the progress through my system of some heavy water (with extra neutrons but not radioactive) they’d had me drink to measure energy expenditure. I had to fill out forms about importation of hazardous chemicals to the USA and arrange for a FedEx courier to collect the package. A rather strange process.
I feel very lucky to have had the opportunity to take part in the study. I hope it proves useful for the research. It provided the inspiration and means for a brilliant holiday with lots of great experiences. Thank you to everyone who I met and who was involved in some way.
A four year old child with sporadic aniridia has raised over £1,000 by walking two miles in aid of Aniridia Network UK (ANUK).
Tora, is blind in one eye and only has peripheral vision in the other. She was joined on the walk near Leeds by her mum Susan, sister, Riley (8), brother Zachariah (1) and 44 other family and friend. Together they raised over £2,00 to share between two charities. You can still sponsor them.
The sun was shining and everyone enjoyed the views, the countryside and playing on sheep sculptures found along the way. Tea and biscuits were kindly provided at the end by Cleckheaton Central
Methodist Church.
Tora was diagnosed with aniridia three days after her birth at Bradford Royal Infirmary. Her parents, Susan and Gordon from Cleckheaton, struggled to find any information about the condition at the hospital. “We were beside ourselves. We didn’t know what it was” said Susan. “Then I ended up speaking to Aniridia Network UK and they explained what it was, what to do and what to look out for – they were really helpful.”
Susan speaking at the ANUK Conference 2012
Since then the Susan and the family have become involved with the charity including being a guest speaker our annual conference in Manchester this year.
Their walk raised money to let ANUK produce a leaflet to put into every hospital for families in the same position as they once were.
It will also fund the Bradford Toy Library at St Luke’s Hospital. It loaned Tora fibre-optic lights to stimulate her eyesight. This local charity has also provided invaluable support to the family through coffee mornings and trips.
“These are the two charities that helped us the most and we would like to raise awareness about the work that they do” said Susan. “Parents can talk to other people who understand the situation they are in. They have been a massive support. ANUK really helped us because we were able to speak to adults who had the condition and share our experiences.”
Susan says Tora “is just like any other young girl. She absolutely loves music, anything from nursery rhymes to Lady Gaga! She is already learning Braille, because we don’t know what will happen in the future to her eyesight, and she is doing really well.” Tora uses a cane and starts school this year.
ANUK Chairperson Katie said “This was a great chance to continue the Paralympic 2012 spirit. We would like to thank Sue, Gordon and Tora for all their hard work raising money for us. We rely on people like them to raise the money we need to keep running each year.”